Key Points
- Medical-grade oxygen is produced via fractional distillation of liquified air and pressure swing absorption.
- Oxygen can be stored as a liquid in vacuum-insulated containers or compressed gas in cylinders.
- Safety systems like the diameter-index safety system and pressure regulators ensure accurate and stable oxygen delivery, making oxygen pipeline system failures rare.
Oxygen Production
- Medical grade oxygen is produced in two ways: fractional distillation of liquified air and pressure swing absorption.1,2
- Fractional distillation consists of two main phases: liquefaction of air and fractional distillation of the liquid air into its components.1,2
- Air is filtered to remove impurities, compressed to remove carbon dioxide and water, and cooled below -170°C to liquefy it. Components are separated based on their boiling points, with nitrogen boiling off before oxygen.1,2
- Separation by fractional distillation is the most common and energy-efficient method for obtaining medical oxygen, resulting in 99% oxygen purity and allowing high-volume production.1
- Pressure swing absorption (PSA) is a technique where pressurized air is passed through nitrogen-absorbing sieves, separating the oxygen from nitrogen.1,2
- Sieves are commonly made of Zeolite, a hydrated aluminum silicate of alkaline earth metals.2
- PSA produces oxygen at concentrations of about 95%.2
- Oxygen concentrators use PSA to produce oxygen. Larger oxygen concentrators can be quickly assembled within healthcare facilities to meet high oxygen demands, particularly if liquid oxygen is unavailable.1,2
Storage of Liquid Oxygen
- Oxygen can be stored as liquid or as compressed gas.
- Liquid oxygen is stored in double-walled steel tanks with an insulating material called vacuum-insulated evaporators.1,2
- To prevent evaporation, liquid oxygen must be stored at temperatures below −183°C, the boiling point of oxygen.1
- Oxygen is withdrawn from the tanks through a vaporizer, where it is heated, vaporized, and distributed as a gas.1,2
- A hospital liquid oxygen storage system includes a main tank, reserve tank, vaporizers, and alarm systems.1
- Hospitals are required to maintain a minimum 1-day supply of oxygen in reserve, achieved through a reserve liquid oxygen supply or a bank of compressed gas cylinders.1,3
- Larger hospitals commonly use liquid oxygen storage systems to improve cost efficiency.1,3
- One milliliter of liquid oxygen provides 860 milliliters of gaseous oxygen at 21 °C and 1 atm.1
Storage of Gaseous Oxygen
• Gaseous oxygen is stored in color-coded cylinders.1,4
o In the United States, green cylinders signify oxygen, while the International Organization for Standardization (ISO) color code for oxygen cylinders is white.1
o Cylinders are commonly made from steel or aluminum but can also be made from composite materials such as Kevlar or carbon fiber.1,2
• The cylinder size is coded alphabetically from A (smallest) to H (largest).1-4
• Some facilities use a newer naming system for medical gas cylinders that begins with “M” for “medical” and is followed by the cylinder’s capacity in cubic feet (Table 1).4

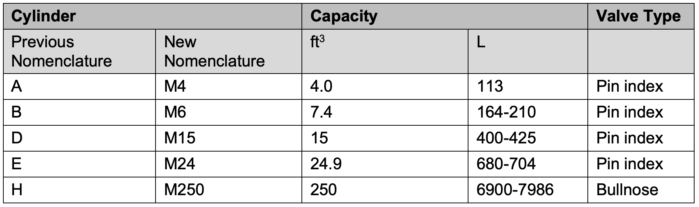
Table 1. Nomenclature and capacities of common medical gas cylinder sizes. Adapted from De Ruyter ML. Medical Gas Supply. In: Trentman TL, Gaitan BD, Gali B, Johnson RL, Mueller JT, Rose SH, Weingarten TN. Faust’s Anesthesiology Review. 5th ed. Elsevier Saunders; 2019:1-3.
- H-cylinders are used for central pipeline supply, particularly in smaller hospitals.3
- For central pipeline storage, oxygen is stored in two separate banks of H-cylinders connected in series by a manifold.2-4
- E-cylinders are used for backup supply and patient transport.4
- Anesthesia machines accept E-cylinders.2-4
- The anesthesia provider is required to have an emergency E-cylinder available during anesthesia delivery.3
- Pressure decreases linearly with oxygen use; for example, an E-cylinder containing 660L of oxygen at 2000 psi will contain approximately 330L of oxygen at 1000 psi.3,4
- The approximate remaining gas flow time of the cylinder can be estimated by the equation: O2 cylinder pressure (psi) / (200 x O2 flow rate [L/min]) = approximate remaining time (h)4
- Service pressure for all cylinder sizes is ~2000 psi.1
- Please check out OpenCriticalCare’s oxygen cylinder size calculator (Link) and cylinder duration calculator (Link).
- Cylinder pressure must be checked before and during use.3
- The Department of Transportation regulates compressed gas storage and transport in the United States, requiring cylinders to have identification marks and labels for gas properties.1,4
- Oxygen cylinders have various safety features, including the hanger-yoke assembly, pin-index safety system, fire safety systems, and pressure relief valves.
- Hanger-yoke assembly: Cylinders attach to the anesthesia machine via this assembly, which orients and supports the cylinder, provides a gas-tight seal, and ensures unidirectional gas flow.3,4
- Pin-index safety system: Prevents cylinder identification errors by ensuring each medical gas has a unique pin configuration on the anesthesia machine’s yoke, aligning holes on the valve block to fit only the correct cylinder (Figure 1). Of note, H-cylinders attach via a “bullnose” fitting, a screw-on fitting not unique to a specific gas type.1,2,4
- Fire safety systems: Cylinders have a plug made from Wood metal, a low-melting-point alloy designed to release pressure in case of a fire.2,3
- Pressure-relief valves: Valves on all oxygen cylinders are designed to release pressure at 3300 psi. A value below the cylinder wall tolerance of ~5000 psi, preventing catastrophic rupture.3
Pipelines and Oxygen Delivery
- Central pipeline oxygen systems supply oxygen from a main liquid oxygen storage tank or H-cylinder bank to hospitals and ORs.
- Gaseous oxygen is delivered to patient care areas through copper-alloy pipes at 50-55 psi.1,3
- Medical gas pipeline systems contain various safety systems, including the diameter-index safety system, pressure regulators, flow meters, and oxygen supply failure protection devices.
- Diameter-index safety system (DISS): Prevents incorrect hose attachment by using noninterchangeable fittings with specific bore diameters for each gas type, ensuring accurate connections and preventing retrograde flow.1,3,5
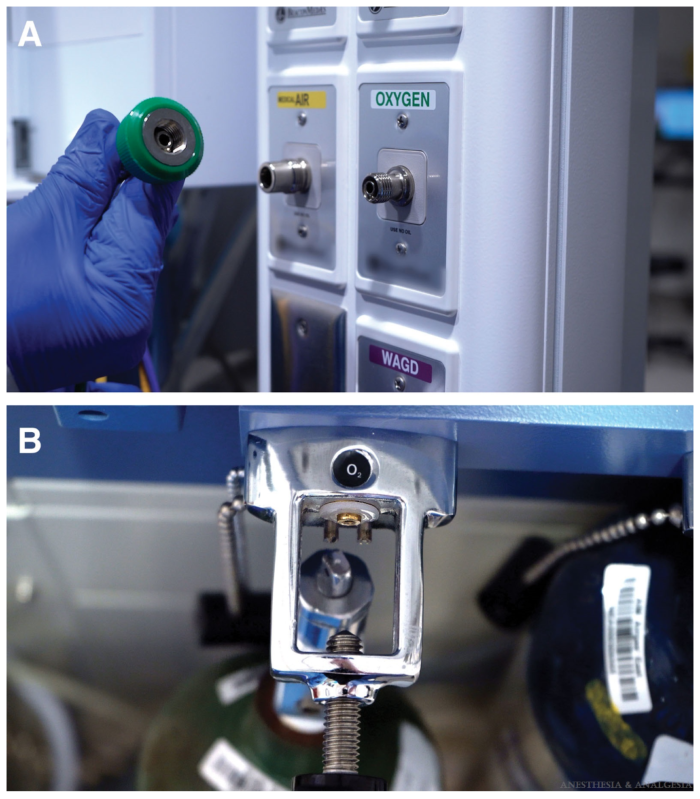
Figure 1. Examples of (A) a diameter-index safety system and (B) a pin-index safety system. Source: Binda DD, Regenbogen I, Nozari A, Ortega R. Hospital oxygen supply: video in clinical anesthesia. Anesth Analg. 2024;138(1):221-225. Link
-
- Pressure Regulators: Reduce high and variable cylinder gas pressures to a stable pressure of approximately 50 psi. Regulators also contain high-pressure relief valves, preventing gas pressures from exceeding the maximum safety limit of 95-110 psi.1,5
- Flow meters: Measure gas flow from the high-pressure to the low-pressure circuit in anesthesia machines. They use color-coded and distinct control knobs to avoid incorrect adjustments. Most modern machines also include features like minimum oxygen flow and oxygen/nitrous oxide ratio controllers to ensure proper gas mixtures and prevent hypoxia.1,5

Figure 2. Example of an oxygen flow meter. Source: Binda DD, Regenbogen I, Nozari A, Ortega R. Hospital oxygen supply: video in clinical anesthesia. Anesth Analg. 2024;138(1):221-5. Link
-
- Oxygen supply failure protection devices: Also known as oxygen pressure alarms, these devices ensure that gases like nitrous oxide and air can only flow if there is adequate oxygen pressure, preventing hypoxic gas mixtures.1,5
Pipeline Failure
- Gas pipeline failures, although rare, have been linked to patient deaths.6
- The most common causes of failure are accidental gas crossover and inadequate pressure.6
- Gas crossover incidents are rare in the United States, secondary to the diameter-index safety system.
- In case of a gas crossover, immediately turn on the backup oxygen cylinder. Disconnect and test the oxygen pipeline before reuse.6
- Inadequate pressure incidents are also rare due to oxygen pressure alarms.
- Loss of oxygen pressure will trigger alarms at 30 psi and then shut off other gas flow below 20 psi. Of note, these systems do not prevent hypoxia due to line misconnections or gas crossover.5
- In case of inadequate pressure, immediately open the backup oxygen cylinder and introduce oxygen from reserve tanks to repressurize the system.6
- If possible, anesthesia should be maintained with volatile agents during oxygen pipeline failures, and backup cylinders should be replaced as needed.6
- Hospital-wide impacts should be assessed, and emergency backup plans initiated, with oxygen supply prioritized for critical patients.6
References
- Binda DD, Regenbogen I, Nozari A, Ortega R. Hospital oxygen supply: video in clinical anesthesia. Anesth Analg. 2024;138(1):221-5. Link
- Das S, Chattopadhyay S, Bose P. The anaesthesia gas supply system. Indian J Anaesth. 2013;57(5):489-99. Link
- The Operating Room Environment. In: Butterworth IV JF, Mackey DC, Wasnick JD. eds. Morgan & Mikhail’s Clinical Anesthesiology, 7e. McGraw-Hill Education; 2022. Accessed August 03, 2024. Link
- De Ruyter ML. Medical Gas Supply. In: Trentman TL, Gaitan BD, Gali B, Johnson RL, Mueller JT, Rose SH, Weingarten TN. Faust’s Anesthesiology Review. 5th ed. Elsevier Saunders; 2019: 1-3.
- The Anesthesia Workstation. In: Butterworth IV JF, Mackey DC, Wasnick JD. eds. Morgan & Mikhail’s Clinical Anesthesiology, 7e. McGraw-Hill Education; 2022. Accessed August 03, 2024. Link
- Weller J, Merry A, Warman G, Robinson B. Anaesthetists' management of oxygen pipeline failure: room for improvement. Anaesthesia. 2007;62(2):122-6. Link
Other References
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.