Key Points
- Gastric point-of-care ultrasound (POCUS) should only be used when the pretest probability of “full stomach” is uncertain.
- Ultrasonography can be used to assess gastric contents by placing the patient in supine +/- right lateral decubitus and scanning with a curvilinear probe to visualize the gastric antrum.
- The gastric antrum is the best target for assessing gastric contents as it dilates in a linear fashion with increased gastric volume and lies in a gravity-dependent location.
- The goal is to sort patients into two categories: (1) low risk of aspiration (Grade 0 or 1 antrum) or (2) high risk of aspiration (Grade 2 or solids).
Indications and Image Acquisition
Indications: when the pretest probability of “full stomach” is uncertain. For example, if the patient is unable to communicate fasting history accurately or is at risk for delayed gastric emptying (e.g., diabetes).
Contraindications: (1) when the presence of gastric contents is already known with reasonable confidence (e.g., a bowel obstruction or alternatively a patient with no gastrointestinal (GI) comorbidities); (2) altered upper GI anatomy (e.g., gastric banding or gastric resection).

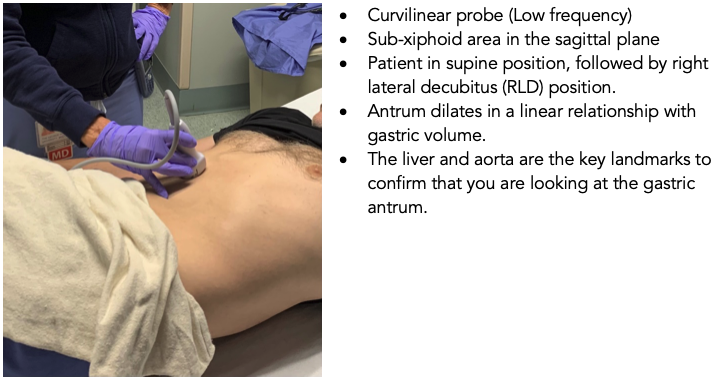
Figure 1. Scanning technique for gastric ultrasound.
Interpretation
It is important to identify the gastric antrum because the antrum dilates in a linear relationship with gastric volume. The antrum of the stomach is identified by the concurrent presence of the liver and abdominal aorta.1,2
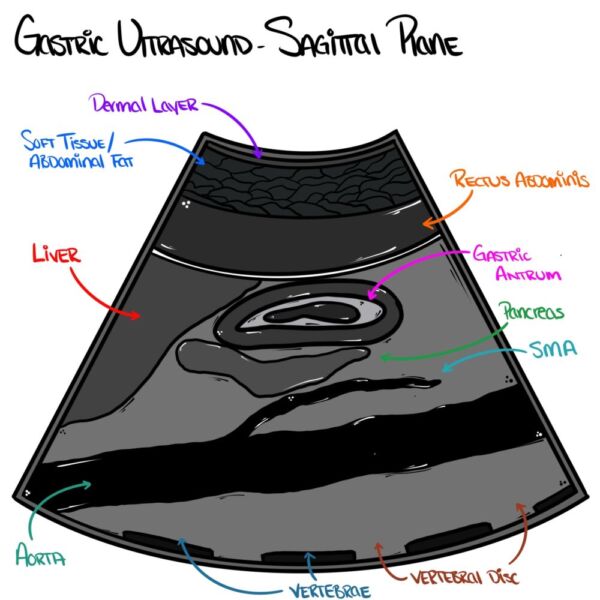
Figure 2. Normal anatomy of the gastric antrum in the sagittal view. The antrum is identified by the presence of two structures in the view: the liver and abdominal aorta. Image reprinted with permission from Countbackwardsfrom10.com.
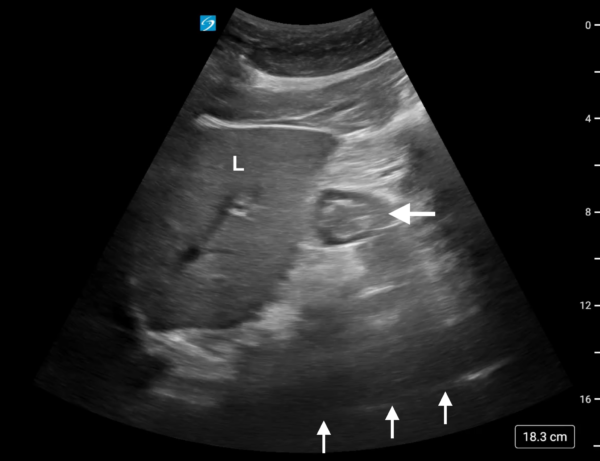
Figure 3. This image of the antrum (horizontal arrow) was obtained with the patient in RLD position after the supine image revealed a completely empty antrum. The combination of an empty antrum in supine position and an empty antrum in RLD position is considered a Grade 0 antrum, which is consistent with a normal, fasted state. Additional structures seen in this image include the liver (L) and abdominal aorta (vertical arrows).
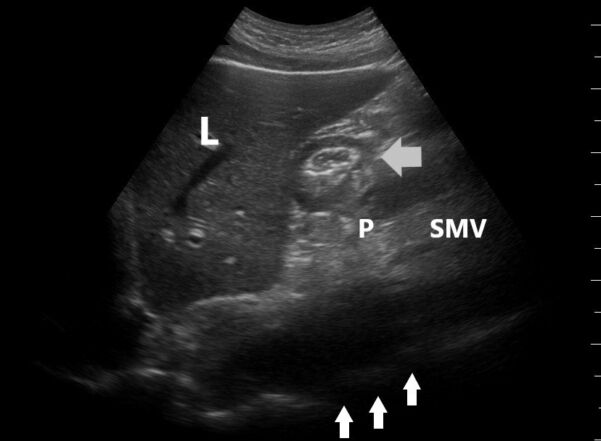
Figure 4. This image was obtained with the patient in RLD position after the supine image revealed a completely empty antrum. The combination of an empty antrum in the supine position and a small amount of clear antral fluid in RLD position is considered a Grade 1 antrum, which is consistent with a normal, fasted state. Additional structures seen in this image include mesenteric vessels (SMV) and pancreas (P).
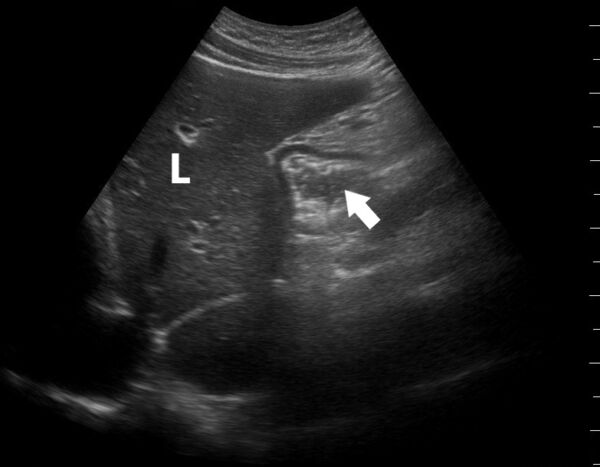
Figure 5. This image of the antrum (arrow) was obtained with the patient in the supine position. The finding of any amount of clear antral fluid in supine position is considered a Grade 2 antrum, which is suggestive of an elevated risk for aspiration.
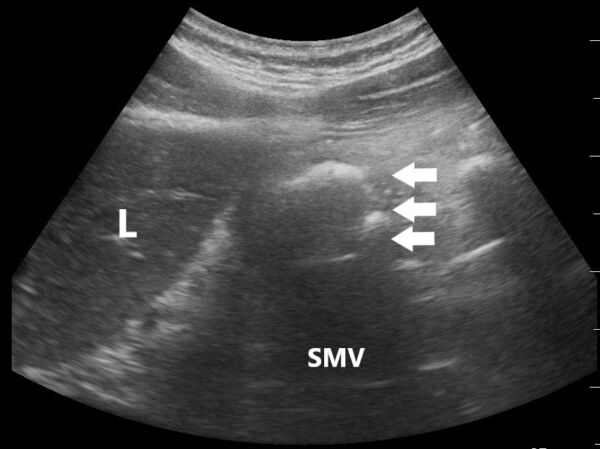
Figure 6. This image of the antrum (horizontal arrows) was obtained in the supine position and shows the findings typical of “early solids.” This pattern is typically seen within an hour after a solid meal. Of note, the anterior wall will appear thickened (top arrow), the lumen has a “frosted glass” appearance (middle arrow), and the posterior wall is distorted (bottom arrow).
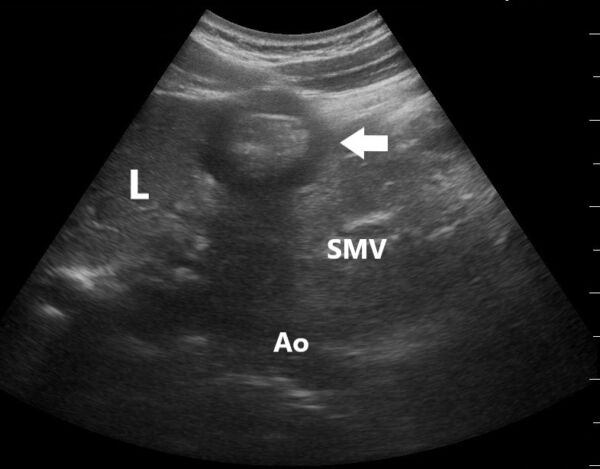
Figure 7. This image of the antrum (horizontal arrow) was obtained in the supine position and is characteristic of “late solids,” which is considered a high risk for aspiration. This pattern is seen a variable amount of time following a solid meal and is characterized by the presence of heterogeneous echogenic material in the antrum and the ability to visualize the posterior antral wall.
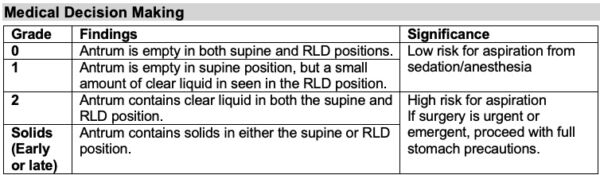
Table 1. Grading of gastric point-of-care ultrasound.1,2
References
- Perlas A, Arzola C, Van de Putte P. Point-of-care gastric ultrasound and aspiration risk assessment: a narrative review. Can J Anaesth. 2018;65(4):437-48. PubMed
- Cubillos J, Tse C, Chan VW, et al. Bedside ultrasound assessment of gastric content: an observational study. Can J Anaesth. 2012;59(4):416-23. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.