The most common patient injuries related to the administration of anesthesia occur due to the failure to recognize a difficult airway. Whereas many tests exist to predict a potentially difficult airway, the sensitivity and positive predictive values of these tests are poor, even in combination. While difficult airways can be devastating for the patient, their rarity makes it difficult to come up with more reliable tests.
It is the responsibility of the anesthesiologist to maintain a patent airway and allow for ventilation after apnea. Failure to accomplish this can lead to catastrophic results including brain injury and death. Thirty percent of all deaths that occur during anesthesia occur secondary to can’t ventilate, can’t intubate conditions. This is why it is imperative for anesthesiologist to recognize and predict difficult airways.
The difficult airway can be represented by difficulty with laryngoscopy, intubation and mask ventilation and is defined as failure to secure an airway after 10 minutes or more than 3 attempts by an experienced anesthesiologist. Before an anesthetic is administered it is important to diagnose potential airway problems and choose alternative modalities of airway management. This starts with a thorough history that highlights issues with intubations in the past, maxillofacial trauma, facial burns or surgery or radiotherapy to the face, neck, pharynx and larynx. The presence of signs such as dyspnea, stridor, dysphagia and snoring strongly correlate with difficult airway as do certain conditions such as obesity, pregnancy, a short neck, prominent maxillary incisors (“buck” teeth), micrognathia, or presence of a beard.
Other disease states that warrant a close airway assessment include hypo- and hyperthyroidism—goiter, infections such as supraglotitis, croup, abscess, Ludwig’s angina, arthritides such as rheumatoid arthritis or ankylosing spondylitis, benign tumors—lipomas, cystic hygromas, adenoma, malignant tumors, acromegaly, acute burns which can cause edema, and syndromes in pediatric population (see table below).

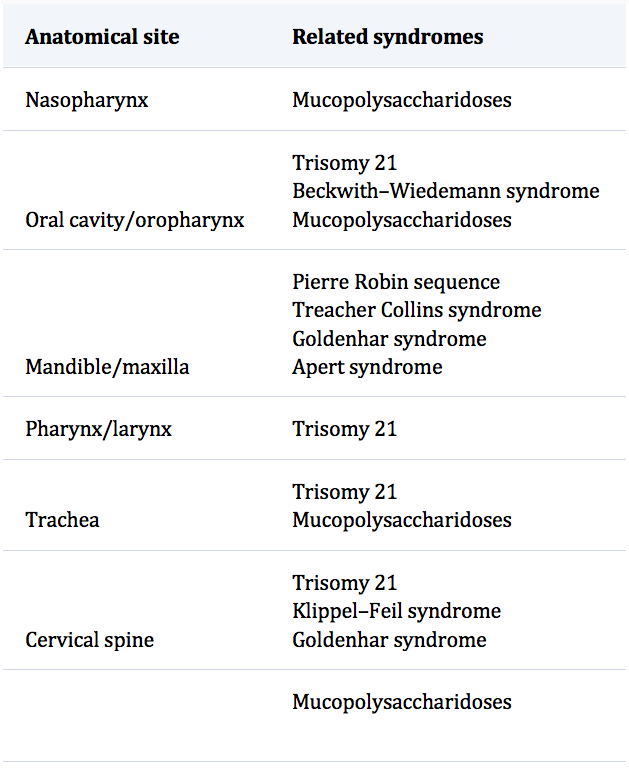
Table: Difficult Airway in Congenital Syndromes Based on Anatomical Site
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.