To understand the potential complications of an ilioinguinal block you must first understand the anatomy. The abdominal wall layers consist of skin, a superficial fatty layer of subcutaneous tissue (Camper fascia), a deep membranous layer of subcutaneous tissue (Scarpa fascia), deep fascia, external oblique muscles, fascia, internal oblique muscles, fascia, transversus abdominus muscles, transversalis fascia, extraperitoneal fat, and finally parietal peritoneum. Depending on body habitus and overall condition, these layers can be quite varied in thickness and strength. Originating from the L1 spinal root, the iliohypogastric and ilioinguinal nerves pierce the transversus abdominus muscle superior and medial to the anterior superior iliac spine. They then run between the transversus abdominus and the internal oblique muscles. In order to block these nerves one can either visualize the layers of the abdominal wall with an ultrasound and deposit local in the correct layer or can use a blunt tipped needle to penetrate the correct layers by feel. In general only about 10-15 ml of local anesthetic, distributed in a “fan-like” pattern is needed for adequate coverage.
Complications:
- Local anesthetic toxicity – this is a risk, but it is very low given the small amount of local needed to perform these blocks
- Hemodynamic changes – highly unlikely given the fact that the block is limited to the lower abdominal wall and inguinal region
- Injury to the anesthetized area – as with any other block the patient must be counseled to avoid trauma to areas that are numb
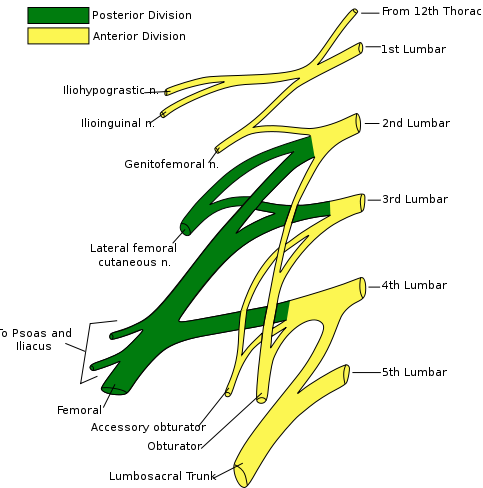
- Later femoral cutaneous or femoral nerve blockade – some of the local anesthetic could track down below the inguinal ligament along the fascia iliaca, giving rise to an unintended block of the femoral nerve. If this occurs the surgical team should be made aware and the patient should be counseled regarding protection of the anesthetized area and the potential for falls.
- Small and/or large bowel perforation – given the close proximity in extremely thin patients and the potential loss of layers or deconditioning of layers of the abdominal wall in older/deconditioned patients, perforation of the bowel is a risk with this block. Blunt tipped needles (compared to sharp needles) help the operator to feel the various fascial layers of the abdominal wall. Care must also be observed in patients with little abdominal wall musculature, because the normal three distinct layers may be too thin to appreciate a loss of resistance between

Other References
- NYSORA: Ilioinguinal and Iliohypogastric Blocks, The New York State School of Regional Anesthesia, Accessed 3/5/15. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.